Members of the project

Project
Group B Streptococcus (Streptococcus agalactiae, GBS) is a natural inhabitant of the gastrointestinal and vaginal flora of 10% to 30% healthy individuals. This Gram positive encapsulated bacterium can also turn into a deadly pathogen in neonates and is recognized as a leading cause of neonatal invasive infections (bacteremia, meningitis). Despite appropriate antibiotic therapy, the global burden of GBS neonatal infections remains substantial, with up to 10% mortality and 30% neurologic sequelae in surviving infants. Two GBS-associated syndromes are distinguished in neonates, the early-onset disease (EOD) which occurs within 48 hr after birth in 90% of the cases, which has substantially decreased with the antibiotic therapy and the late-onset disease (LOD) which occurs between 7 and 89 days of life. The mode of transmission and the infection route of LOD, characterized by a bacteremia without focus and a high rate of associated meningitis, remain elusive, and although the gastrointestinal tract represents the most likely portal of entry, the circumstances leading to LOD remain largely unknown. Worldwide epidemiological data have identified that GBS strains are distributed among five major clonal complexes (CC). One particular GBS clone, almost exclusively of capsular serotype III and designated the hypervirulent CC17 clone, is strongly associated with LOD (60% to 80% of the cases) and with meningitis (approx. 80% of the cases). CC17 GBS expresses specific surface proteins which promote intestinal colonization and confer blood brain barrier (BBB) translocation abilities in animal models. Remarkably, this clone is less responsible for EOD and largely underrepresented in GBS adult diseases implying that specific host factors might be involved in CC17 GBS invasiveness in >7 day-old neonates.
This project is focused on the intestinal barrier crossing by GBS CC-17 clone.
The project is divided into two complementary axes. On the one hand, we define the interactions between SBG and the intestinal barrier and, on the other hand, we are interested in the bacterial environment of GBS in the intestine.
Interactions GBS - intestinal barrier
One particular aspect of the perinatal life is the very high concentration of pregnancy-related hormones, especially estradiol (E2) and progesterone (P4), to which neonates are exposed all along pregnancy. This hormonal exposure leads to neonatal circulating concentrations at birth which are more than 500 times superior to those of a male adult. These levels drop during the first 3 days of life to stabilize for several months at concentrations still 5 to 50 times higher than those of an adult. Interestingly, sex hormones modulate the immune response and the permeability of cellular barriers in a dose-dependent manner. Thus, E2 and P4 concentrations found at a given time-period of the neonate’s development could promote GBS and more particularly CC17 GBS invasiveness and LOD.
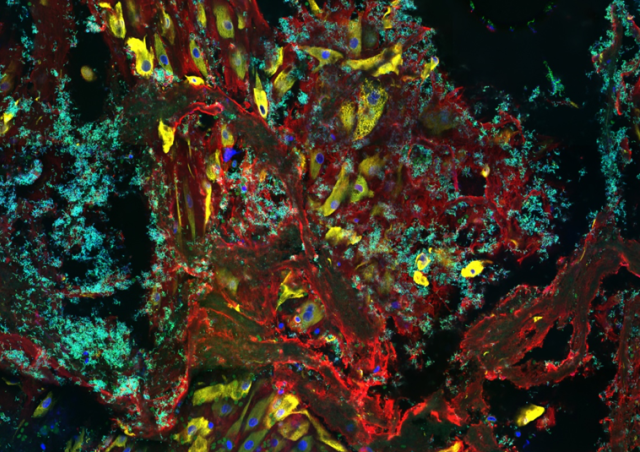
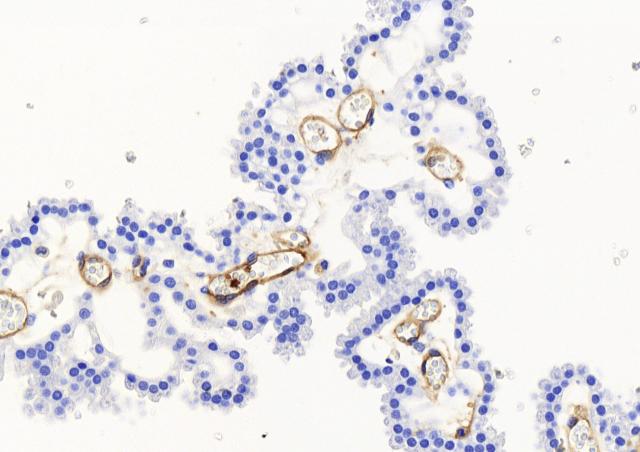
Using an approach combining murine and cellular models of infection with one CC17 and one non-CC17 representative GBS isolates, both of capsular serotype III and responsible for neonatal disease, we demonstrate that hormonal exposure to E2 and P4 concentrations found in 7-day-old neonates (E2-P4 C7) specifically favors CC17 GBS pathogeny in comparison to E2 and P4 levels found at birth (E2-P4 C0). The increased invasiveness of CC17 GBS in E2-P4 C7 condition is linked to an enhanced crossing of the intestinal barrier through M cells which is mediated by the CC17-specific surface protein Srr2.

Metagenomics and perinatality
In France and industrialized countries, almost half pregnant women and their newborns are administered an antibiotic prophylaxis or therapy during delivery for the prevention of early-onset neonatal bacterial infection, including GBS infection. This antibiotic therapy can have mid to long-term consequences on microbiota establishment and composition and on immune system development. This project aims at analyzing the microbiota associated to neonatal colonization by GBS together with the impact of environmental factors such as antibiotic administration and the feeding diet on microbiota composition.
Our research interests are:
- Identify the metagenomics signatures of neonatal colonization par GBS and especially by CC-17 GBS at 3 weeks and 2 months of age. This will allow the development of novel preventive approaches against CC-17 late-onset disease, including a better identification of neonates at risk for infection and direct targeting of the gut microbiota.
- Investigate the impact of intrapartum antibiotics on maternal vaginal microbiota and on the composition and functions of the neonate’s intestinal microbiota. Metagenomics, metabolomics and immunological approaches will be used to correlate metagenomics signatures to various functions of the microbiota.
- Identify vaginal microbial communities associated with pregnancy complications and neonatal infection. The impact of vaginal dysbiosis and of pathobionts on premature rupture of outer membranes is studied.
Publications
Funding